Myasthenia Gravis
Myasthenia Gravis: Pathophysilogy,clinical features, diagnosis and management
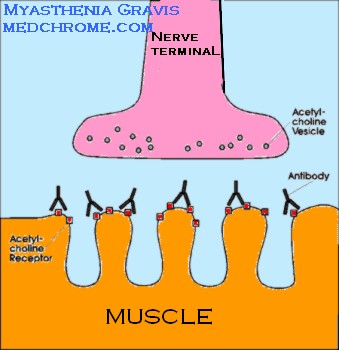
It is a Neuromuscular disorder characterized by weakness and fatigue of the skeletal muscles. It occurs as a result of decreased number of Acetyl Choline receptors ( AcHR) in post-synaptic muscle membrane. It is Antibody mediated Autoimmune disorder.
Pathophysiology :-
Anti AcHR antibodies activates the complement that cause Autoimmune reaction that destroys the AcHRs at muscle endplates. This results in low endplate potential which fails to trigger muscle action potential. Thus , there is failure of neuromuscular transmission and weakness of Muscle contraction occurs.

Thymus is suggested in the pathogenesis of MG. It is known to play a role in initiation and maintainance of Autoimmune response. Abnormal Thymus is found in75% of such cases. Thymic hyperplasia in 65% patients. Thymoma is present in 10% of patients.
Muscle Specific Kinase Antibody ( MUSK)
Clinical Features:-
- Prevalence rate worldwide is 1 in 7500 population.
- Peak Incidence women in 20s and 30s, Men in 50s and 60s.
- Women: Man Ratio is 3:2
- Cardinal Signs are:-
- Weakness and Fatiguability Of Muslces
- Worse with repeated activity
- Improved by Rest.
- Exacerbation and Remission occurs during early years
- Cranial muscles , lid and extraocular muscles are involved early
- Diplopia and Ptosis are the results.
- Weakness in Chewing, Swallowing and Speaking.
- Generalized weakness in 85% affecting limb muscles
- Limb weakness is often proximal and may be asymmetrical.
- Respiratory muscles may be involved- In case of Myasthenia Crisis
- Deep tendon reflexes are intact.
Investigations:
1 Autoimmune Test:-
Edrophoniumis used in Tensilon test. 2 mg IV initial dose cause improvement ion muscle power within 30 seconds and persists for 2-3 minutes. Further dose of 8 mg if no improvement.
2. EMG ( ElectroMyogram):
Repetitive nerve stimulation shows characteristic decremental response. Rapid reduction in amplitude of evoked muscle action potential of more than 15%.
3.Antiacetylcholine Receptor Antibody:
Definite diagnosis if positive but Negative result does not exclude the disease.
4.Antiskeletal Muscle Antibody:
Positive suggests the presence of Thymoma.
5.CT, MRI:- for ocular or cranial MG to exclude Intracranial lesions.
6. Exclude Other disease- PFT, TFT, RA factor, ANA, Antithyroid Ab
Disorders associated with MG:
- Disorders of thymus, thymoma,hyperplasia
- Other Autoimmun disorders- Thyroiditis, Graves disease, RA, SLE etc
- Medical treatment with Aminoglycosides and Quinine may aggravate the disease.
Diffrential Diagnosis:-
- Lambert –Eaton MG ( LEMG)
- Neurothenia
- Hyperthyroidism
- Botulism
- ICSOL
Management:-
Principles-
- To maximize the activity of AcH in remaining receptos in NMJ
- To Limit or abolish the immunological attack on the motor endplates.
- Anticholinesterases: Pyridostigmine 30-120 mg QID
It prolongs the action of AcH
- Immunological treatment of MG:
Thymectomy
Plasma Exchange
Intravenous Immunoglobins against AcH Ab
Corticosteroids
Other Immunosuppresants.

4 Comments
Good Post. Better then the simillar post I found last Wednesday on Blogspot
Does anyone know who his neurologist was? My father has been detected with it.
I heard Amitabh Bacchan had Myasthenia .
He is under treatment.
Yes, AMitabh Bacchan was diagnosed with Myasthenia gravis.
Comments are closed.