Carpal Tunnel Syndrome: Features and Treatment
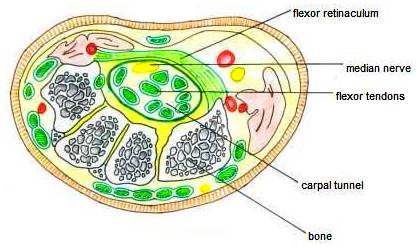
Anatomy of Carpal Tunnel:
Carpal tunnel is a narrow passageway in the wrist formed by:
Posterior side: 8 carpal bones
Anterior side: Transverse carpal ligament
Contents:
9 Flexor tendons
Median Nerve
Median Nerve Distribution in Hand:
Origin: From lateral and medial cords of brachial plexus
Motor innervation:
Lumbricals: 1st and 2nd
Muscles of thenar eminence: Opponens pollicis, Abductor Pollicis Brevis and Flexor Pollicis Brevis)
Mnemonic: LOAF (Lumbricals, Opponens pollicis, Abductor Pollicis Brevis and Flexor Pollicis Brevis)
Sensory innervation:
Skin of the palmar side of the thumb, the index and middle finger, half the ring finger, and the nail bed of these fingers (3 and 1/2 digits)
Lateral part of the palm by palmar cutaneous nerve (unaffected in Carpal tunnel syndrome)
Carpal Tunnel Syndrome
It is a syndrome characterized by the compression of the median nerve as it passes beneath the flexor retinaculum in carpal tunnel.
Causes:
Any space occupying lesion (SOL) of carpal tunnel can cause carpal tunnel syndrome –
Inflammatory causes:
- Rheumatoid arthritis
- Wrist osteoarthritis
Post-traumatic causes:
- Colle’s fracture
Endocrine causes:
- Myxoedema
- Acromegaly
Idiopathic
Mnemonic: MEDIAN TRAP
- Myxoedema
- Edema premenstrually
- Diabetes
- Idiopathic
- Acromegaly
- Neoplasm
- Trauma
- Rheumatoid arthritis
- Amyloidosis
- Pregnancy
Clinical features:
It usually occurs in females between the age of 40 and 70. They complain of tingling, numbness or discomfort in the lateral 3 and 1/2 fingers i.e. distribution of median nerve. They also complain of intermittent attacks of pain in the distribution of the median nerve on one or both sides. The attacks frequently occur at night. The reason symptoms are worse at night may be related to the flexed-wrist sleeping position and/or fluid accumulating around the wrist and hand while lying flat. Pain may be referred proximally to the forearm and arm.
Motor changes: Ape-like thumb deformity, loss of opposition of thumb, index and middle fingers lag behind when making the fist
Sensory changes: Loss of sensations on lateral 3 and 1/2 digits including the nail beds and distal phalanges on dorsum of hand
Vasomotor changes: The skin areas with sensory loss is warmer due to arteriolar dilation; it is also drier due to absence of sweating due to loss of sympathetic supply
Tropic changes: Long-standing cases of paralysis lead to dry and scaly skin. The nails crack easily with atrophy of the pulp of fingers.
Tests
To approximate where along the wrist the median nerve runs, gently flex and radially (laterally) deviate your wrist. Two tendons will become palpable and even visible—palmaris longus (in midline) and flexor carpi radialis
(lateral to it). However, 15% of people do not have a palmaris longus muscle. The median nerve runs deep between these tendons.
Phalen’s Test:
Bend the patient’s wrists downwards as shown in the figure
This position should be held for about 1 minute.
Positive test : numbness or tingling along the median nerve distribution
Tinel’s Test:
With the palm up, tap over the carpal tunnel area of the wrist 5 or 6 times
Positive test : tingling or paresthesia in the median nerve distribution
Durkan Test:
Press thumb over carpal tunnel and hold pressure for 30 seconds.
Positive test: Onset of pain or paresthesia in the median nerve distribution
Nerve conuction studies are done for diagnosis these days
Treatment

- Immobilizing braces/Splints
- Analgesics like NSAIDs
- Local injection of steroids
- Surgery: Dividing the flexor retinaculum
Carpal Tunnel Syndrome as Occupational Disease
Causes:
- repetitive hand motions
- awkward hand positions
- strong gripping
- mechanical stress on the palm
- vibration
Common occupations:
- Cashiers
- Hairdressers
- Knitters
- Farmers (milking cow)
- Office workers (keyboarding)
- Painter, etc.
12 Comments
I hva nagging pain in my index finger of right hand which irigintes at forearm History of carpal fracture 60 years back .Advise tretment and diagnosis Could it be carpal tunnel?
Certainly it can be carpal tunnel syndrome, fractures are likely cause, along with many other causes. Get a neurologist review, you may need NCVS.
I have an irregular sharp pain between thumb joint and forefinger joint on that edge of palm. The pain is relieved sometimes by stretching thumb & forefinger. The pain first appeared about 2 years ago when opening very tight lid of new jamjar of large diameter. Do I have CTS?
Thanks. Rich
It may be Skier’s thumb or arthritis as well. You should get it checked.
Can cts be caused by twisting of the wrist when lifting a heavy object , Also are sharp pains a symptom?
Thank you, Mike
Twisting of the Wrist usually results in Tenovaginits which is inflammation of common sheath of 2 tendons ( APB and EPL) muscles in forearm which is characterized by sharp pain when thumb is jerked with another hand.
im suffering from my hand pain numbness ang tingling pls help me what can i do>thank u
Hand pain and numbness may not always be Carpel Tunnel Syndrome, but CPS very likely, get an appointment with a doctor. You need to rule out other neurological causes, vascular causes or bony cause if you have history of fractures in the past.
my pain is coming from the base of my thumb is that carpal tunnel
The pain at base of Thumb may be due to-
De Quervian’s Tenovaginitis
Features seen in DQ TV are-
Clinically
Commonly – women aged 40 – 50 years
pain on the radial side of the wrist ( thumb finger side)
Tenderness at base of thumb
May feel crepitus = wet leather sign
Pain on stretching the thumb.
Arthritis of the joint ( 1st metacarpophalangeal joint)
Carpal Tunnel Syndrome
These 3 are likely causes, but for proper diagnosis you should consult an Orthopedic doctor and get it treated.
two things : current research does NOT support correlation with computer/keyboarding as a cause
second: Not Agromegaly, it is Acromegaly
Thanks for the update TJ,
Comments like your can help us as well as the readers.
Keep it up
Research say CTS is less in intense keyboard users
http://www.ncbi.nlm.nih.gov/pubmed/17968917
Comments are closed.