Acute Appendicitis Made Easy
ANATOMY OF APPENDIX
Because of the variation in position, the appendix is said to be the only organ in the body without anatomy. However, the anatomy of vermiform appendix has been discussed in detail here.
ETIOLOGY
1. White race > Dark race; Young males; Middle class and rich
2. Diet rich in meat and lacking cellulose
3. Long retrocecal appendix (due to diminished blood supply)
4. Luminal obstruction: fecolith, ball of worms (oxyuriasis vermicularis), lymphoid hyperplasia, foreign objects, stricture (tumor)
5. Non-obstructive: Bacterial (E.coli, Enterococci, Proteus, Pseudomonas, Klebsiella, anaerobes) and Viral infection
TYPES
1. Mucosal: Mildest
2. Phlegmonous: Slow onset and relatively slow progression
3. Necrotic: Acute bacterial infection with ischemic necrosis → Perforation
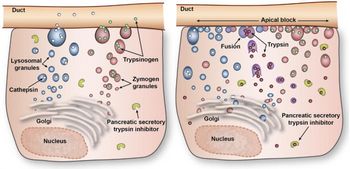
PATHOGENESIS

CLINICAL FEATURES
 A. Symptoms:
A. Symptoms:
1. Murphy’s triad (Pain → Vomiting → Fever):
a. Shifting pain: Severe colicky periumbilical visceral pain (common T10 innervation for both appendix and umbilicus – referred pain) which later migrates to right iliac fossa (somatic pain due to inflammation of parietal peritoneum)
Somatic phase of pain is based on anatomy of appendix:
- Long tip: Left lower quadrant (LLQ) pain
- Retrocecal/Retrocolic: Right Flank or back
- Pelvic: Suprapubic pain
- Retroileal: Testicular pain (from irritation of spermatic artery and ureter)
- Pregnancy: Right upper quadrant (RUQ) pain (if appendix is shifted)
b. Vomiting (1-3 times/day): Vomiting occurs after pain in contrast to gastroenteritis which is opposite to appendicitis.
c. Fever
2. Others:
- Diarrhea (May be mistaken for gastroenteritis)
- Pyuria / Hematuria (May be mistaken for UTI)
- Facial flushing
B. Signs:
Mnemonic: ABC OPqRST

1. Aaron’s sign: Pain or pressure in epigastrium or anterior chest with persistent firm pressure applied to McBurney’s point.
2. Blumberg sign: Rebound tenderness at McBurney’s point
3. Cough tenderness: Differentiates from right sided ureteric colic
4. Obturator (Cope’s obturator) sign: Flexion and medial rotation at hip produces pain due to irritation of obturator muscle in pelvic appendicits.
5. Psoas (Cope’s psoas) sign: Pain in attempt to extend the hip flexed due to irritation of psoas major in retrocecal appendicitis)
6. Rigidity and Guarding in Right Iliac Fossa (RIF)
7. Rovsing sign: Palpation of left iliac region → Displacement of colonic gas and small bowel towards inflamed appendix → Pain on right iliac region
8. Rectal examination: Tenderness in right rectal wall
9. Sherren triangle hyperaesthesia: Area of skin hyperaesthesia bounded by bounded by lines joining anterior superior iliac spine, the pubic symphysis and umbilicus.
10. Ten Horn sign: Pain caused by gentle traction of right testicle
ALAVARADO SCORING SYSTEM
Mnemonic: MANTRELS
The score for the features are indicated in the bracket which on total makes 10.
Symptoms (MAN):
- Migrating RIF pain (1)
- Anorexia (1)
- Nausea and vomiting (1)
Signs (TRE):
- Tenderness RIF (2)
- Rebound tenderness (1)
- Elevated temperature (1)
Laboratory (LS):
- Leukocytosis (2)
- Shift to left i.e Neutrophilia (1)
Anaylsis of score:
- < 5 : not sure
- 5-6: compatible
- 6-9: probable
- >9: confirmed
TZANAKIS SCORING SYSTEM
- Right lower abdominal tenderness : 4 points
- Rebound tenderness : 3 points
- Presence of white blood cells greater than 12,000 in the blood : 2 points
- Presence of positive ultrasound scan findings of appendicitis : 6 points
A total score of 15 is the maximum that can be scored. Where a patient scores 8 or more points, there is greater than 96 percent chance that appendicitis exists.
DIFFERENTIAL DIAGNOSIS (RLQ PAIN)
Mnemonic: APPENDICITIS
- A : Appendicits
- P : PID , Period/Menstruation (Female)
- P : Parasites (Oxyuriasis – children, Amoeba – young adults), Pancreatitis (Middle age), Pelvic kidney
- E : Endometriosis and Ectopic pregnancy (Female), Enterocolitis (children)
- N : Neoplasia (Ca. cecum)
- D : Diverticulitis (Children and Young adults), Duodenal ulcer (Middle age)
- I : Iliac lymphadenitis and Intusussception (Children)
- C : Cystic ovary (Female), Cholecystitis (Middle age)
- I : IBD (Chron’s disease)
- T : Torsion of undescended testis (Young adults)
- I : Irritable Bowel Syndrome
- S : Stones
Systemic Diseases (6 P)
- Pleurisy
- Pneumonia
- Porphyria
- Pott’s spine
- Preherpetic pain
- Purpura
INVESTIGATIONS
To support our clinical diagnosis, following investigations will help:
A. Laboratory:
- Total WBC count: Leukocytosis 10,000 to 18,000/cu.mm (If >18,000/cu.mm, consider perforation with or without abscess)
- Urinananalysis: Several WBCs and RBCs may be found in appendicitis secondary to bladder irritation from inflamed appendix.
- Elevated CRP (C-reactive protein)
B. Diagnostic Imaging:
- Abdominal X-ray (may reveal fecolith): to rule out perforation
- Abdominal USG (+ve if >6mm noncompressible appendix): to rule out gynecological pathology
- Laproscopy: to rule out ovarian pathology in females
- Abdominal CT scan
CT scan is costly and one need to keep the economic status of patient in mind before sending this investigation.

COMPLICATIONS
1. Rupture (Perforation) → Generalized peritonitis
- Increased risk in infants (thin omentum without much fat) and elderly (atherosclerosis of appendicular artery which is an end-artery)
2. Appendicular mass: cecum, terminal ileum and appendix sealed by greater omentum
3. Appendicular abscess
4. Others: Adhesions, Portal pyaemia, Abdominal actinomycosis
TREATMENT
1. Definitive treatment: Appendicectomy or Appendectomy (Open or Laproscopic)
2. Appendicular mass: Appendicectomy is contraindicated as it may lead to fecal fistula. Hence, we opt a conservative treatment (Oscher and Sherren’s regime – ABCDEF).
- Aspiration (with Ryle’s tube)
- Bowel care (purgatives shouldn’t be use due to risk of perforation)
- Charts (Temperature, Pulse, Respiration, Mass size)
- Drugs (Antibiotics to cover all gram positive, gram negative and anaerobe organisms)
- Exploratory laparotomy (Only in suspicion of abscess)
- Fluid I.V (To correct dehydration)
The patient is kept in close observation and within 3-4 days if:
- Symptoms resolve: Interval appendicectomy after 6-8 weeks
- Symptoms progress: Urgent appendicectomy with or without drainage
3. Appendicular abscess: Drainage is performed depending on the site –
- Retrocecal: RIF incision → Extraperitoneal approach
- Pre- and Post-ileal: Laparotomy
- Lumbar: Loin incision
- Pelvic: Transrectal approach


4 Comments
Wow beautifully explained…
This topic is excellently presented.
Thanks
This is one of the best explanation on any topic I’ve tried to find out…Thanks so much and I hope to see more of it in the filed of medicine.
sir this is a nice discription on appendicites. I think some more picture are discribe well. but it nice. thanks.
Comments are closed.