
Epistaxis
Background:
Epistaxis, or bleeding from the nose, is a common complaint. It is rarely life threatening but may cause significant concern. Most nosebleeds are benign, self-limiting, and spontaneous, but some can be recurrent.
Epistaxis can be divided into 2 categories, anterior bleeds and posterior bleeds, on the basis of the site where the bleeding originates.
N.B
Important anatomy to know
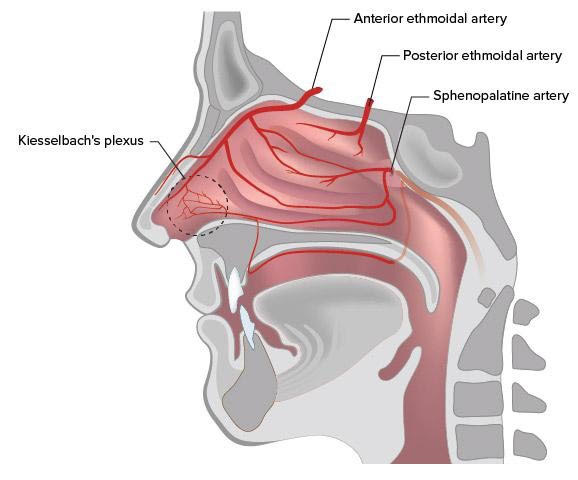
The nose has a rich vascular supply, with substantial contributions from the internal carotid artery (ICA) and the external carotid artery (ECA).
The ECA system supplies blood to the nose via the facial and internal maxillary arteries. The superior labial artery is one of the terminal branches of the facial artery. This artery subsequently contributes to the blood supply of the anterior nasal floor and anterior septum through a septal branch.
The internal maxillary artery enters the pterygomaxillary fossa and divides into 6 branches: posterior superior alveolar, descending palatine, infraorbital, sphenopalatine, pterygoid canal, and pharyngeal.
- The Kiesselbach plexus, or Little’s area, is an anastomotic network of vessels located on the anterior cartilaginous septum. It receives blood supply from both the ICA and the ECA. Many of the arteries supplying the septum have anastomotic connections at this site.
Etiology:
- local causes (eg, trauma, mucosal irritation, septal abnormality, inflammatory diseases, tumors)
- systemic causes (eg, blood dyscrasias, arteriosclerosis, hereditary hemorrhagic telangiectasia),
- Idiopathic causes the cause of epistaxis is not always readily identifiable. Approximately 10% of patients with epistaxis have no identifiable causes even after a through evaluation.
Complications:
- Sinusitis.
- Septal hematoma/perforation
- External nasal deformity
- Mucosal pressure necrosis
- Vasovagal episode
- Balloon migration
- Aspiration
Clinical spots:
Ask specific questions about the severity, frequency, duration, and laterality of the nosebleed. Determine whether the bleed occurs after exercise or during sleep or is associated with a migraine. Determine whether hematemesis or melena has occurred because posterior bleeding in particular may present in this fashion. Foreign bodies inserted in the nose may also present with epistaxis, but bleeding may be less and accompanied by foul or purulent discharge if the object has been retained for some time. A unilateral nasal discharge suggests the presence of a foreign body.
Inquire about previous epistaxis, hypertension, hepatic or other systemic disease, easy bruising, or prolonged bleeding after minor surgical procedures. A history of frequent recurrent nosebleeds, easy bruising, or other bleeding episodes should make the clinician suspicious of a systemic cause and prompt a hematologic workup. Obtain any family history of bleeding disorders or leukemia.
Use of medications—especially aspirin, NSAIDs, warfarin, heparin, ticlopidine, and dipyridamole—should be documented, as these not only predispose to epistaxis but make treatment more difficult. Particularly in children, include investigation of suspicion of accidental ingestion (eg, accidental ingestion of rat poison in toddlers).
Management and treatment:
1 – Initial treatment begins with direct pressure. The nostrils are squeezed together for 5-30 minutes straight, without frequent peeking to see if the bleeding is controlled. Usually, 5-10 minutes is sufficient.
Patients should keep their heads elevated but not hyperextended because hyperextension may cause bleeding into the pharynx and possible aspiration. This maneuver works more than 90% of the time.
{ If direct pressure is not sufficient, Do with epinephrine or phenylephrine }
2 – Nasal packing can be used to treat epistaxis that is not responsive to cauterization. Two types of packing, anterior and posterior, can be placed. In both cases, adequate anesthesia and vasoconstriction are necessary.
3 – Electro-cauterization
4 – Arterial ligation The choice of the specific vessel or vessels to be ligated depends on the location of the epistaxis. In general, the closer the ligation is to the bleeding site, the more effective the procedure tends to be.
Medication
Most patients with epistaxis who seek medical attention are likely to be treated with cauterization, anterior packing, or both. Those with severe or recalcitrant bleeding may need posterior packing, arterial ligation, or embolization. Pharmacotherapy plays only a supportive role in treating the patient with epistaxis.
“As antibiotics, anesthetics and topical vasoconstrictors.”
The following precautions should be imparted to the patient:
- Use nasal saline spray.
- Avoid hard nose blowing or sneezing.
- Sneeze with the mouth open.
- Do not use nasal digital manipulation.
- Avoid hot and spicy foods.
- Avoid taking hot showers.
- Avoid aspirin and other NSAIDs.
The following simple instructions for self-treatment for minor epistaxis should be provided:
- Apply firm digital pressure for 5-10 minutes.
- Use an ice pack.
- Practice deep, relaxed breathing.
- Use a topical vasoconstrictor.
Reference:
Quoc A Nguyen, Associate Clinical Professor, Director, Sinus and Allergy Center, Department of Otolaryngology-Head and Neck Surgery, University of California, Irvine, Medical Center
Author bio:
Mostafa. M. H. Haredi is a 4th year medical student in Minya Uni., Egypt.
He says – “I am a member or EMSA (Egyption Medical Students Association) which aims to help students to learn and how to research. I have published a question bank book for veterinary students and perparing for a clincal spots in anatomy. I’d like to help anyone want to know and learn”.