
Spinal Anesthesia: Anatomy, Physiology, Technique, Contraindication and Complication
 Spinal anesthesia, also known as Subarachnoid blockade or Spinal block is a type of regional anesthesia in which the lower half of the body is anesthetized by injecting an anesthetic agent in the subarachnoid space surrounding the spinal cord.
Spinal anesthesia, also known as Subarachnoid blockade or Spinal block is a type of regional anesthesia in which the lower half of the body is anesthetized by injecting an anesthetic agent in the subarachnoid space surrounding the spinal cord.
A. Indications:
- Transurethral prostatectomy (a block to T10 is required because of innervation of the bladder)
- Hysterectomy
- Hernia repair
- Caesarean section (block to T6)
- Evacuation of retained products of conception
- Any procedure on the lower limb such as major joint replacement
- Other pelvic and perineal procedures
In general, indications of spinal block are lower abdominal surgery, lower limb surgery and perineal surgery.
B. Advantages:
- Cost effective
- Patient satisfaction
- Few adverse effect on respiratory system
- Patent airway
- Diabetic patients can usually return to their normal food and insulin regime soon after surgery as there is less sedation, nausea and vomiting.
- Excellent muscle relaxation for lower abdomen and lower limb surgery.
- Decreased blood loss due to decreased Blood pressure and heart rate, and improved venous drainage.
- Increases splanchnic blood flow, reducing the risk of anatomic dehiscence.
- Lower risk of postoperative Deep vein thrombosis and Pulmonary emboli.
C. Position: Lumbar puncture for Spinal anesthesia may be performed in either the sitting or the lateral decubitus position.
D. Anatomical Considerations:
The spinal cord terminates at L1-L2 in adults (L3 in infants) and the dural sac extends down to S2 (lower in children). Therefore, the subarachnoid space between L2 and S2 contains only CSF and lumbar and sacral nerve roots (cauda equina). The line joining the iliac crests (intercristine or Tuffier’s line) is at the L3/L4 interspace. If there is any doubt about the level then the space below should be chosen to prevent inadvertent needle insertion in the L2/L3 interspace which may lead to entry in the cord or the conus medullaris leading to intense pain and possible permanent damage to the cord. The subarachnoid space is approximately 6 cm from the skin surface in a person of average build. The order of the structures pierced by the needle before it reaches the subarachnoid space: skin, subcutaneous tissue, supraspinous ligament, interspinous ligament, ligamentum flavum, epidural space and dura. A click can be felt as the dura is pierced, and the patient may complain of paresthesia in the lower extremities at the same time. A local anesthetic solution injected deposited in the lumbar subarachnoid space can travel caudad and cephalad to provide anesthesia for operations on the perineum, the external genitalia, the lower extremities and abdominal organs.
E. Approach:
After positioning the patient, L3-4 interspace is identified using a landmark (Tuffier’s line) and a skin wheal is raised at the center of the interspace. Insert a 22-29 G needle of your choice.
- Midline: at the level of the interspace, insert a needle in the midline. With 15 degree cephalad angulation, advance until a click or pop is felt, at an approximate depth of 4-6 cm.
- Paramedian: 1-2 cm lateral to the upper border of the spinous process. Insert a needle perpendicular to the skin to contact the lamina of the vertebra. Withdraw slightly, reinserting the needle 15 degree medially and 30 degree cephalad to pass over the lamina through the interlaminar space. Advance until a click or pop is felt due to piercing of the dura.
After free flow of CSF inject the desired volume of anesthetic agent.
Types of Needle:
- Quincke (cutting) end hole
- Whitacre/Sprotte (splitting) side hole ‘pencil point’
F. Drugs used:
The usual agent used for Spinal anesthesia is Bupivacaine 0.5%.
- Heavy: Hyperbaric bupivacaine formulated in a 5% glucose solution, increasing its density, which may make it fall under gravity to dependent parts of the subarachnoid space. The usual duration of the block is 2-3 hours. Due to spread in the intrathecal space, heavy solutions can be used to achieve a higher block.
- Plain: Isobaric bupivacaine will usually produce a lower block height (T12-L1) with consequently less hypotension under normal conditions.
Other local anesthetics: Lignocaine, Xylocaine, Tetracaine, Mepivacaine, etc.
Small doses of lipid-soluble opioids (eg. diamorphine) are often added to the mixture to prolong the duration of analgesia postoperatively.
Ketamine can also be used to supplement spinal anesthesia in low doses.
G. Physiology of Spinal anesthesia:
Site of action: Spinal nerves and dorsal ganglia minimally on spinal cord
Differential blockade: The sequence of block is autonomic (sympathetic) fibers first,then sensory fibers and lastly motor fibers. Sympathetic block may extend as many as 2-6 dermatomes higher than pin-prick sensation, which in turn extends to 2-3 dermatomes higher than motor block. This spatial separation is believed to result from a gradual decrease in local anesthetic concentration within the CSF as a function of distance from the site of injection.
H. Factors increasing the number of affected spinal segments:
- Higher dose
- Higher volume
- Pregnancy (Due to smaller subarachnoid space and venous congestion)
- Increase in abdominal pressure
- Head-down tilt of the patient
- Coughing or straining by the patient during or immediately following injection
- Barbotage (a technique in which the CSF is repeately withdrawn into the syringe during the course of injection to promote mixing)
I. Contraindications:
1. Absolute:
- Local sepsis
- Patient refusal
- Anticoagulation
2. Relative:
- Aortic stenosis/mitral stenosis (profound hypotension – sympathetic block)
- Previous back surgery (technical difficulty)
- Neurological disease (medicolegal)
- Systemic sepsis (increased evidence of epidural abscess, meningitis)
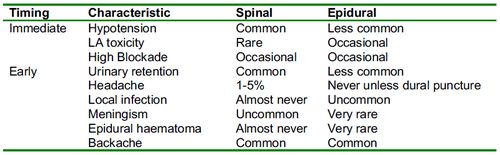
J. Complications:
1. Hypotension:
- Cause: Vasodilation resulting from sympathetic block (higher the block the more widespread the vasodilation)
- A very high block (upper to T4) may directly affect cardio-accelerator fibers arising from the upper thoracic cord leading to bradycardia exacerbating the hypotension.
- Treatment: Intravenous fluid, Ephedrine, Atropine
2. Post-dural puncture Headache:
- Cause: Traction effect due to CSF leak
- Nature: Throbbing front-occipital headache, worse on standing and relieved by lying down
- Treatment: Simple analgesics, Encouragement of oral fluids or use of intravenous fluids, Caffeine, Autologous blood patch or Normal saline patch (Last resort)
3. Rare complications:
- Labyrinthine disturbance
- 6th cranial nerve disturbance
- Meningitis
- Transverse myelitis
- Cauda equina syndrome
References:
- Churchill’s Pocketbooks Anaesthesia – Nathanson and Mahajan
- Oxford Handbook of Anaesthesia 2nd edition – Allman and Wilson
- Essentials of Anesthesiology – Chung and Lam
- Spinal Anaesthesia “A practical guide” – Ankcorn and Casey
thanks, i like it.