
Case Review : Acute ST Elevation MI
A 46 years Male from Nuwakot came to ER with complains of Epigastric and retrosternal pain for 16 hours. The pain was constricting type , continuous, radiating to left arm and neck, and not relieved in any position. It was associated with Shortness of breath. He had 3 episodes of Vomiting and sweating. He also complains of palpitation. Headache +, LOC followed the event and he was rushed to ER. Bowel/Bladder habits were Normal.
He had no history of chest pain before but he is a smoker, 9-10 sticks per day for past 30 years. He occasionally consumed alcohol.
He doesn’t give history of HTN, or Diabetes Mellitus.
On Examination at ER:
- GC- patient conscious but in agony.
- Vitals- Blood pressure- 100/80 mmHg, Pulse= 64/minute, RR=32/min , Temperature=Normal
- Cardinal signs- JVP- raised
- Chest- Bilateral Normal Vesicular Breath Sound, No added sounds
- CVS- S1 and S2 Normal, No mumur
- P/A- soft, non-tender, no organomegaly
- ECG showed- ST-T changes specific of Antero-lateral Myocardial Infarction. Q waves.

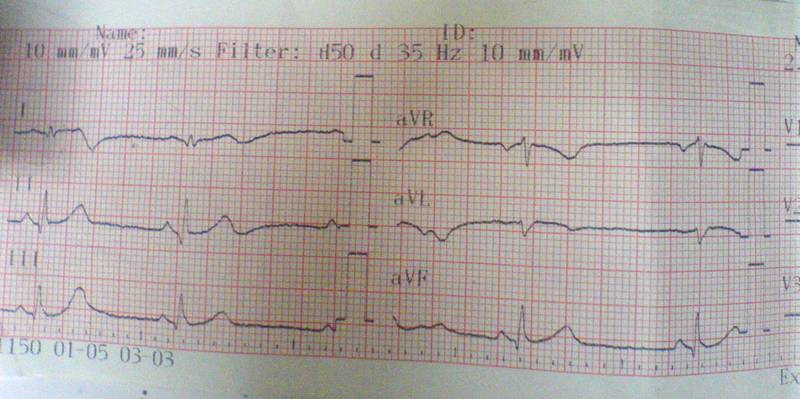{kind=link}

- Total Count- 11,700 with N-87 and L-10, Hemoglobin=13.4 g%
- Cardiac Enzymes= CPK MB= 109 U/L after 4 hours CPKMB=421U/L, Troponin I was positive.
Diagnosis- Anterolateral MI
Immediate Management-
- Oxygen
- Aspirin
- Clopidogrel
- Inj Morphine
- LMW Heparin
- Isosorbide dinitrate
- Isosorbide Mononitrate
- Alprazolam
- Cremaffin
Patient could not be Thrombolysed because it was past recommended time and Q waves in ECG were seen by arrival.
CCU course-
day1 -Patient developed hypotension . ECG showed Inferior wall extension.Inotropes were started.
day 2-Couplets were seen, Hr-120 beats/min and was controlled by beta-blocker Metoprolol low dose
day 3- Inotropes were tapered gradually. Patient’s condition improved.
ECHO done.
Planned for Coronary Angiography. Possible CABG.
- Acute Myocardial Infarction : Read Text Review here
- Acute Coronary Syndrome: Read