
Anencephaly : A severe Birth defect
Anencephaly- Clinical features, pregnancy diagnosis, prevention and treatment.

Spina Bifida and anencephaly are most common Neural Tube Defect ( NTD) followed by encephalocele. Anencephaly is a severe form of NTD, with 100% mortality. The baby is either born dead or is unfit for survival.
Anencephaly is a congenital birth defect (from the Latin congenitus, “born with”)
Incidence Of Anencephaly: 1 in 1000 children ( world statistics, exact for Nepal is not available). In USA data is 1 in 150,000 to 200,000 babies born each year are anancephalic .
Cause Of Anencephaly:
- The anomaly results from deficient development development of the vault of skull and brain tissue due to incomplete closure of the Rostral Neuropores.
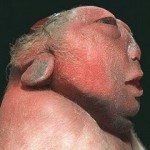
Clinical Features
- The facial portion is present. Infants with this disorder are born without a scalp or cerebellum. Their meninges, both hemispheres of the brain and the vault of the cranium/skull are also missing, though they usually do have part of the brain stem. The remaining brain tissue is protected only by a thin membrane.
- About ¼ of anencephalic babies die at birth; those who survive have a life expectancy of a few hours or days
- A baby born with anencephaly is usually blind, deaf, unconscious, and unable to feel pain. Although some may be born with a main brain stem, the lack of a functioning cerebrum permanently rules out the possibility gaining consciousness.
- Reflex actions such as breathing and responses to sound or touch occur.
- The pituitary gland is often absent or if present is hypoplastic. Secondary to absence of stimulation in absence of ACTH , pituitary glands are also atrophied.
Risk Factors:
- Previous history of birth of infant with NTD
- 70 % of the cases are female .
- It is most common in first birth and among young and elderly mothers.
- Genetic and environmental factors are suspected to be involved.
Diagnosis Of Anencephaly:
- In the first half of pregnancy, the diagnosis is made by elevated Alpha-fetoprotein in Amniotic fluid and confirmed by sonography. The findings around 13 weeks gestation are:- Absence of Cranial vault, Angiomatous brain tissue.
- In later half of pregnancy, the diagnosis may be a problem. Hydraminous and inability to palpate fetal head can arouse suspicion.
- Face presentation is revealed by internal examination ( per vaginum).
- Confirmation is done by USG or X ray.
Complications:
- Hydramnios
- Malpresentation – face or breech
- Premature labour
- Tendency to post-maturity
- Shoulder dystocia
- Obstructed labour – if head and shoulder present (compound) due to short neck
Management:
- If diagnosed before 20 weeks of pregnancy: Termination of Pregnancy is done
- If Diagnosed Late: PGE2 (Cerviprim gel can be used to to terminated the pregnancy as Uterus is usually resistant to Oxytocin.
- If Diagnosed During labor- The labor is likely to be prolonged. For Shoulder dystocia- Cleidotomy should be done. ( Cutting the clavicle bones)
Prevention Of Anencephaly:
- Pre-pregnancy Counselling is important.
- Folic Acid supplementation 4 weeks before the conception to 12 of pregnancy has reduced the incidence of NTD significantly. A dose of 4 mg daily is recommended.
- Regular follow up visits Antenatal.
- Mothers on drug ( Antiepileptics) should consult the doctor.
Gallery:

Source : DC Dutta Obstetrics book, Wikipedia, www.anencephalie-info.org .