
Viral hepatitis genotyping: a tool for therapeutic management
Viral hepatitis – a group of infectious diseases known as hepatitis A, B, C, D, and E – affects millions of people worldwide, causing acute and chronic liver disease and killing close to 1.4 million people every year. The WHO assembly meeting held on 28th July, 2014 reaffirmed viral hepatitis as a global epidemic and agreed to intensify efforts to prevent, diagnose and treat such infections. The resolution recognizes the great potential of new medicines and treatment approaches for chronic hepatitis C and hepatitis B infection, calling for cost-effective strategies to increase access in middle- and low- income countries where its needed the most.
The incidence of HCV on a global scale is not well known, because acute infection is generally asymptomatic. But worldwide, more than one million new cases of hepatitis C virus (HCV) infections are reported annually. In India, about 12 million are infected with HCV. Of these, 80% patients develop chronic infection (with damaged liver), 20% will develop fatal liver cirrhosis over a few years and 5% will suffer from liver cancer (fig. 1).1 Similarly, hepatitis B virus (HBV) is another major global public health problem and is the 10th leading cause of death worldwide. An estimated 350 million individuals are chronically infected with HBV and approximately 1 million die annually. India has a HBV surface antigen carrier rate of 2-7% in general population and is classified as a region of intermediate HBV endemicity.2
The ultimate goal is a universally effective vaccine to prevent new cases, especially in underdeveloped countries, where hepatitis infections are more prevalent and treatment is financially out of reach for most patients. The development of such a vaccine has been hampered, at least partly, by the great heterogeneity of the hepatitis genome, which is the focus of this review.
Fig 1. Proportion of HCV-infected patient as per disease severity in India.
Hepatitis C virus infection
The hepatitis C virus (HCV) is a RNA virus belonging to the Flaviviridae family and consists of at least 6 major HCV genotypes (each comprising multiple subtypes). The long-term impact of HCV infection is highly variable, ranging from minimal histological changes to extensive fibrosis and cirrhosis with or without hepatocellular carcinoma (HCC). The primary goal in HCV treatment is to achieve undetectable HCV RNA in patient plasma samples 24 weeks after therapy (defined as sustained virological response, SVR), indicative of resolution of liver disease without cirrhosis. Patients who fail to achieve an SVR are at a risk of life threatening conditions.
Until 2011, prior to the approval of direct-acting antivirals (DAAs) like telaprevir and boceprevir, the combination of pegylated interferon (PegIFN)-alpha and ribavirin for 24 or 48 weeks was the approved treatmentfor HCV infections. With this regimen, patients infected with different HCV genotypes achieved variable SVR rates: genotypes 2, 3, 5,and 6 (up to 80%), genotype 1 (40-50%) and genotype 4 showed intermediate SVR rates. Following the introduction of DAAs, improved SVR rates (65-75%) were observed in patients infected with genotype 1. This raised the hopes for the use of IFN-free regimens; but the clinical acceptance of DAAs was limited due to its severe side effect profiles especially in patients with advanced hepatic fibrosis. Hence, IL28B genotyping due to its predictive value was useful in categorizing patients who could be treated only with PegIFN-alpha and ribavirin; thereby limiting their exposure to DAAs.3
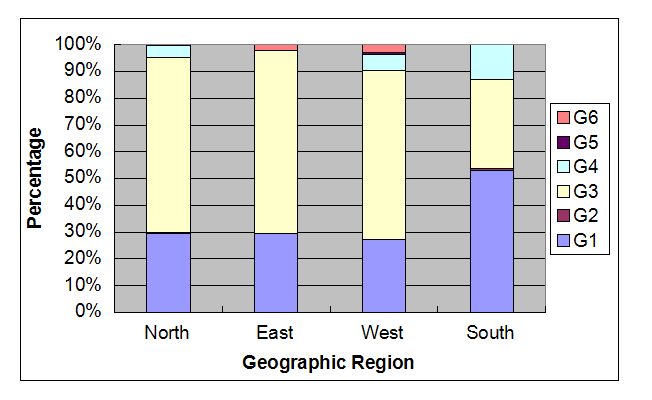
In 2014, second generations of DAAs found to be more efficacious and clinically tolerable (in patients with advanced liver disease) were approved for clinical use. These drugs reported improved SVR rates across all HCV-genotypes (independent of host IL28B genotype) along with decrease in treatment duration. Clinical trial studies have documented genotype 2/3 infected patients to achieve an SVR rate of 80-95% within 12-24 weeks; while patients with genotype 1 infection achieved an SVR rate of 82-100% within 12 weeks of therapy. Thus, an immediate shift towards IFN-free regimens has been observed in settings without any economic constraints. Recent guidelines have recommended the use of DAAs for anti-HCV treatment; but its usage and treatment duration is highly dependent on the viral genotype.3 Hence, determination of HCV genotype before initiation of treatment plays an important role in effective patient management. Two major protocols exists for determination of viral genotype: line probe hybridization and sequencing (the gold standard). A study from SRL (data unpublished) using the sequencing methodology have performed HCV genotyping on 6674 specimens (2012-2014), and found that genotype 3 was highly prevalent across India (except the Southern region, genotype 1 was predominant), followed by genotype 1 (figure 2). Similar results have been reported by other studies across different geographical regions of India.4
Fig 2. represents the prevalence of HCV genotypes across different geographic regions of India.
Hepatitis B virus infection
HBV disease can occur as an acute infection (typically observed in infected adolescents or adults who have not been vaccinated) and chronic infection (acquired in early childhood and associated with high levels of viral replication with few or no clinical symptoms). Progression of chronic HBV infection to severe liver diseases are usually a result of both host- and viral- characteristics; and without intervention, 15% to 40% of chronic HBV-infected individuals will develop cirrhosis, end-stage liver disease, HCC, or will require liver transplantation.2
Although, HBV viral load and presence of drug resistance conferring mutations have a direct impact on the patient clinical outcome; recently viral genotypes are also known to influence patient treatment outcomes. HBV is naturally heterogeneous with 10 genotypes (A-J) that differ genetically by greater than 8% (and 4-8% for subtypes). Each genotype is predictive of viral characteristics, disease severity progression and response to interferon therapy (Table 1).5 Hence, accurate identification of HBV genotype is of significant clinical importance in effective patient management.
Table 1. Clinical influence of different HBV genotypes.
| Genotype | B | C | A | D | E-J |
| Mode of transmission | Vertical | Vertical | Horizontal | Horizontal | Horizontal |
| Tendency of chronicity | Lower | Higher | Higher | Lower | Not determined |
| Clinical outcomea | Better | Worse | Better | Worse | Worse in genotype F |
| Response to interferon therapy | Higher | Lower | Higher | Lower | Lower in genotype G |
| Serum HBV DNA level | Lower | Higher | Not determined | Not determined | Not determined |
Source: Reference 5
aClinical outcome, measure of disease severity progressing towards cirrhosis and hepatocellular carcinoma.
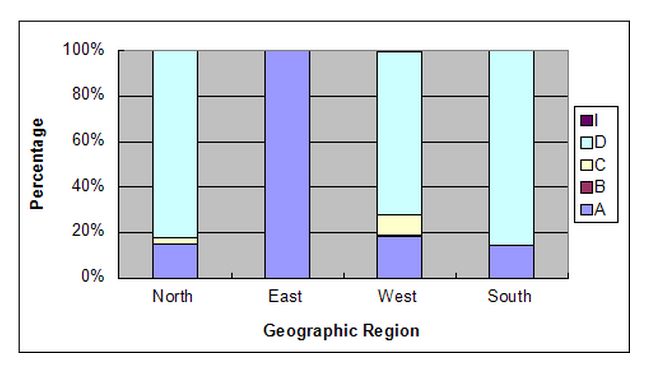
There are a number of methods available for determination of HBV genotype: Restriction Fragment Length Polymorphism analysis, type-specific PCR, real-time PCR, line probe hybridization and sequencing (the gold standard). Each of these methods target the pre-S region (higly variable region) of the viral genome capable of differentiating individual HBV genotypes. A study from SRL (data unpublished) using the sequencing methodology have performed HBV genotyping on 264 specimens (2012-2014), and found that genotype D was found to be highly prevalent, followed by genotype A and genotype C (figure 3). Although a small sample size, but an important observation was complete dominance of genotype A HBV infections in East region of India.
Fig 3. represents the prevalence of HBV genotypes across different geographic regions of India.
References
-
DNA: Daily News and Analysis. Hepatitis C drug: From Rs 1.8 crore to Rs 1.2 Lakh. http://www.dnaindia.com/mumbai/report-hepatitis-c-drug-from-rs-18-crore-to-rs-12-lakh-2073038 Last accessed on 13th July, 2015.
-
Sibnarayan Datta. An overview of molecular epidemiology of hepatitis B virus (HBV)in India. Virology J.2008;5:156.
-
European Association for the Study of the Liver. EASL Recommendations on Treatment of Hepatitis C 2015. J Hepatol (2015), http://dx.doi.org/10.1016/j.jhep.2015.03.025;in press.
-
Mukhopadhya A. Hepatitis C in India.J. Biosci. 2008;33:465-473.
-
Lin CL, Kao JH..The clinical implications of hepatitis B virus genotype:Recent advances. J Gastroenterol Hepat. 2011;26(1):123-130.
Authors Profile


President-Research & Innovation,
Mentor-Molecular Pathology and
Clinical Research Services
SRL R&D, Mumbai