
Diagnosing Abdominal Tuberculosis: Current recommendations
Abdominal tuberculosis (TB) is a collective term that includes TB of the gastrointestinal tract, peritoneum, omentum, mesentery and its lymph nodes and other abdominal organs such as liver, spleen and pancreas. Its presentation has dramatically changed with increasing incidence of HIV coexistence, making the diagnosis in HIV infected persons quite challenging. Also, abdominal tuberculosis can mimic a variety of other abdominal conditions/diseases; hence clinical acumen and timely use of appropriate diagnostic modalities play a very important role in preventing morbidity and mortality.
Types of abdominal TB
Gastrointestinal TB is the commonest form, with the ileocecal area being the most commonly involved site. Majority of these cases have associated lymph node and peritoneal involvement. Lymph node TB in the abdomen is mainly mesenteric or retro-peritoneal. Peritoneal involvement occurs in 4-10% cases and is usually a result of hematogenous seeding or direct spread from ruptured lymph nodes and intra-abdominal organs. Peritoneal TB can present as adhesions or ascites. Infection of solid organs such as liver, spleen and pancreas mainly occurs due to disseminated/miliary tuberculosis.

Abdominal TB can present at any age but is more commonly seen in young adults.
Manifestations that raise clinical suspicion of abdominal TB
Clinical manifestations vary from asymptomatic disease to acute, acute on chronic or chronic symptomatic disease. Individuals can present with a myriad of symptoms depending up the site of infection.
Typical site specific clinical manifestations can include:
- Intestinal – Recurrent intestinal colic, partial or complete intestinal obstruction, chronic diarrhoea, unexplained weight loss, palpable mass in lower abdomen, lower GI bleeding.
- Abdominal Lymph node TB – Dull or colicky abdominal pain, abdominal distension,weight loss, night sweats or fever, and evidence of abdominal lymphadenopathy on abdominal ultrasound scan, CT or MR
- Peritoneal – Abdominal distension, abdominal pain, fever
- Perianal – perianal fistulae, persistent discharge from the fistula, recurring fistulae sfter multiple surgical excisions.
- Hepatobiliary – Fever of unknown origin, hepatomegaly with or without space occupying lesions, abnormal LFTs (especially elevated alkaline phosphatase), abnormal imaging (abscess, space occupying lesions), jaundice
- Pancreatic – Abdominal pain, and/or obstructive jaundice, and/or dilated pancreatic and/or bile ducts with evidence of (peri)-pancreatic mass or cyst with or without constitutional symptoms
- Oesophageal – Dysphagia, odynophagia, hematemesis, constitutional symptoms
- Gastroduodenal – Gastric outlet obstruction, upper GI bleeding
Abdominal tuberculosis often mimic other conditions such as
- Malignant neoplasms,
- Inflammatory bowel disease
- Cirrhosis of the liver (especially peritoneal tuberculosis)
Hence differential diagnoses must always be carefully evaluated. In fact , hepatobiliary, pancreatic, oesophageal /gastroduodenal manifestations are more likely to be diagnosed as malignancies as compared to TB.
Diagnosis: Current guidelines for India
All patients with presumptive abdominal TB must be subjected to a chest X-ray examination to look for primary focus. Also, since Extrapulmonary TB is often associated with HIV infection, all individuals should be offered HIV counseling and testing.
Appropriate specimens from the presumed site of involvement must be obtained for laboratory based diagnosis. Common tests include AFB microscopy/culture, Validated NAAT / GenXpert(CBNAAT) , Cytology /Histopathology examination. The basic principle of seeking bacteriologic diagnosis at every opportunity where TB is suspected is to be followed. Extrapulmonary TB diagnosis is more challenging than pulmonary TB, due to paucibacillary nature of disease. Hence, this site specific specimen may need to be subjected to a combination of tests, in order to overcome sensitivity/specificity related limitations of individual tests.
Ascitic fluid sampling can aid in the diagnosis of peritoneal TB. Specimens should be sent for: a) cytology; b) albumin and protein; c) adenosine deaminase (ADA); d) AFB microscopy / Culture. A serum albumin: ascitic fluid albumin ratio (SAAG) of <1.1 with a high protein (>2.5 g/mL) is suggestive of an exudative process, in keeping with abdominal TB (although several other conditions also cause this). High ADA levels are also suggestive of abdominal TB. AFB microscopy/culture have relatively low sensitivity on ascitic fluid, nevertheless culture is required to confirm the diagnosis and test for drug susceptibility. NAAT based methods can give variable results in terms of diagnostic accuracy.
Ultrasound guided FNAC or core biopsy of mesenteric/retroperitoneal lymph nodes, omentum or peritoneum can be subjected to histology & AFB microscopy/culture. Sensitivity of microbiology tests is higher with FNAC/biopsy specimens than ascitic fluid testing alone.
Abdominal Ultrasound/CT/MR scan are valuable to study the pathognomonic abnormalities, including intra-abdominal fluid , lymphadenopathy, bowel wall thickening, strictures, enlarged lymph nodes with central necrosis, and peripheral enhancement and peritoneal and omental thickening. However none of the findings are diagnostic for peritoneal TB. These tests may be useful when other differential diagnoses are being considered.
Laparoscopy is not routinely recommended due to invasive nature of the procedure, and is usually reserved for cases where the diagnosis remains unclear after other tests. Laparoscopy can reveal typical appearances that are highly suggestive of peritoneal TB. Targeted diagnostic sampling at laparoscopy may improve the yield from biopsy specimens sent for Histopathology, AFB microscopy and culture.
For patients with suspected intestinal TB, patients should be offered endoscopic examination with appropriate biopsy sampling for Histopathology, AFB microscopy and culture. Examination of the ileum by retrograde ileoscopy is important. Differentiating TB from other bowel diseases such as Crohn’s disease can pose a challenge on endoscopy.
In case of upper GI involvement, barium studies of the upper GI tract and small bowel may be indicated where endoscopy is not available or not possible, or where small bowel stricture is suspected.
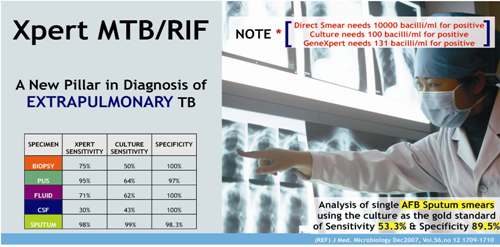
Role of Xpert MTB/RIF (GenXpert) in abdominal TB diagnosis
Xpert MTB/RIF is a commercial PCR based diagnostic test for detecting genetic material specific to M. tuberculosis and rpoB gene that confers resistance to Rifampicin. The test has high accuracy for diagnosing pulmonary TB. Studies however show that the test may have lower sensitivity in extrapulmonary specimens. Hence recent guidelines deem it inappropriate to recommend Xpert MTB/RIF as the principle diagnostic test. Nevertheless, considering the benefit it offers in terms of rapid diagnosis , Xpert MTB/RIF can be used as an additional test to microscopy, culture and cytology in FNAC specimens. A systematic review has shown Xpert’s pooled sensitivity & specificity to be 83.1% and 93.6% respectively, for lymph node TB. A negative Xpert MTB/RIF test does not rule out TB.
AUTHOR:-

References:
- WHO & CTD, MOHFW GOI. INDEX-TB GUIDELINES – Guidelines on extra-pulmonary tuberculosis for India 2016
- Chugh S , Jain V. Medicine update-Chapter 102: Abdominal Tuberculosis — Current Concepts in Diagnosis and Management.600-8