The diagnosis Human Immunodeficiency Virus (HIV) infection leading to Acquired Immunodeficiency Syndrome (AIDS) was considered as a death sentence a few decades ago. Advents in diagnosis, monitoring and therapy, have dramatically reduced HIV related mortality and morbidity.
The use of HIV medicines to treat HIV infection is called antiretroviral therapy (ART). ART involves taking a combination of HIV medicines (called an HIV regimen) daily. ART has been proven to reduce the HIV viral load and substantially boost the capacity of immune system. ART cannot cure HIV infection, but it can help people infected with HIV live longer, healthier lives. HIV medicines can also reduce the risk of transmission of HIV.
The drugs currently used to treat HIV-1 infection belong to different classes such as:
Nucleoside Reverse Transcriptase (RT) Inhibitors (NRTIs) and Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs) which act on reverse transcriptase, an enzyme HIV needs to make copies of itself
Protease(PR) Inhibitors (PIs) which block HIV protease, an enzyme essential for HIV replication
Fusion and entry inhibitors which prevents entry of HIV in the CD4 cells
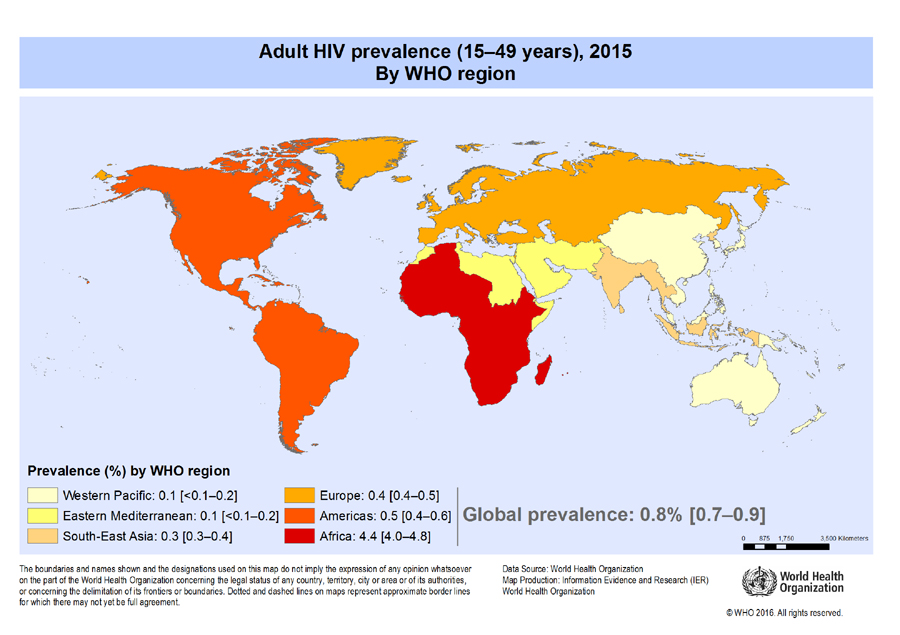
The National AIDS Control organization (NACO) of India introduced the National ART program to provide free treatment to HIV- infected individuals in 2004. Out of the 37 million people living with HIV (PLHIV) globally in 2015, around 2.1 million are from India. India is estimated to have around 86 (56–129) thousand new HIV infections in 2015, showing 66% decline in new infections from 2000. This decline is consistent with the rapid expansion of access to ART in the country. It is estimated that the scale-up of free ART since 2004 has saved cumulatively around 4.5 lakhs lives in India until 2014.
What is HIV drug resistance?
Once a person becomes infected with HIV, the virus begins to multiply in the body. As HIV multiplies, it sometimes mutates (changes form) and produces variations of itself. Variations of HIV that develop while a person is taking HIV medicines can lead to drug-resistant strains of HIV. HIV medicines that previously controlled the person’s HIV are not effective against the new, drug-resistant HIV and can’t prevent the drug-resistant HIV from multiplying. The consequences of HIV-DR include treatment failure leading to illness and death and further spread of drug resistant HIV.
Evolution of Drug resistance:
A person can initially be infected with drug-resistant HIV or develop drug-resistant HIV after starting HIV medicines. There are numerous factors that result in the development of drug resistant strains of the virus. Firstly, HIV has a high replication rate with the process of reverse transcription of viral RNA into DNA being highly prone to error. This results in the generation of different quasi-species of HIV being present in the same individual, each differing by one or more mutations. This may lead to changes in the specific molecular targets to which the drugs bind, such as enzymes or receptors, leading to ineffective action of ART and emergence of drug resistant HIV strains.
The second factor,adherence to ART, remains the most important and definitely the most preventable factor contributing to the development of resistance. If the drug levels in the blood vary due to lack of adherence to treatment or impaired drug absorption, any of these naturally occurring mutations can confer some selective advantage to the virus, resulting in multiplication of drug resistance strains over the drug sensitive wild type of virus.
Combination therapy can minimize the emergence of drug resistance as multiple drugs suppress viral replication more effectively than single agents and multiple mechanisms are required to encode resistance to different classes of drugs. Hence, standard HIV treatment regimens across the world recommend the use of at least two classes of drugs simultaneously.
Global Impact:
Around 17 million people worldwide are receiving ART. With an ambitious aim to end the AIDS epidemic by 2030, UNAIDS has launched the 90-90-90 strategy in 2014; by 2020, 90% of all people living with HIV will know their HIV status, 90% of all people with diagnosed HIV infection will receive sustained ART and 90% of all people receiving ART will have viral suppression. A stepping stone to achieve this target, the new guidelines from WHO in 2015 strongly recommend that for all adults ART should be initiated regardless of WHO clinical stage and at any CD4 count. New studies have evidenced that early initiation of ART has decreased HIV related illness and death and reduced the risk of HIV transmission. But as greater number of people with HIV will receive ART, the problem of drug resistance is expected to increase, which may undermine the impressive gains made by global programs in halting the progress of the AIDS epidemic.
HIV-DR results in more rapid virological failure (increase in viral load) with first line therapy. Second line therapy has to be initiated for patients with HIV-DR strains. The second line therapy is more expensive and has increased adverse effects which may lead to poorer adherence. This may result in higher mortality and morbidity.
Diagnosis of HIV DR:
In order to limit the emergence of resistance to ART, HIV treatment should be accompanied by periodic virological and genotype monitoring. CD4 counts are impacted after viral load increases and hence monitoring viral load provides an earlier indication of drug resistance. With ART being started irrespective of CD4 counts, viral load monitoring is now recommended by WHO as the preferred monitoring approach.
When plasma viral load increases in spite of therapy, it is of essence that ART should be changed quickly. The appropriate selection of second line treatment is of great importance as HIV may show cross resistance to different drugs in the same class or even to different classes of drugs. If the patients do not respond to the prescribed ART regimen and worsening clinical symptoms are suggestive of HIV drug resistance, it is of paramount importance to suspect and diagnose treatment failure.
Genotypic resistance testing evaluating the susceptibility of HIV to individual retroviral therapy is recommended before switching the treatment regimen. Most genotypic assays involve sequencing of the RT and PR genes to detect mutations that are known to confer drug resistance. Interpretation of test results requires knowledge of the mutations selected by different antiretroviral (ARV) drugs and of the potential for cross resistance to other drugs conferred by certain mutations. Prompt testing helps to select the most effective second line drugs and thereby minimize the morbidity and mortality associated with HIV-DR. Timely changes in treatment regimen based on genotypic drug resistance testing results may prove to be life saving decisions in clinical management.
As the inevitable consequence of expanded ART coverage, HIV drug resistance is an emerging threat to the global efforts for containing and eliminating the HIV epidemic. Taking cognition of this, WHO has now begun developing a global action plan to support a coordinated international effort to prevent, monitor and respond to the emergence of HIV drug resistance, and to strengthen country efforts to achieve the global HIV targets. Educating patients about the importance of adherence to treatment regimes and alert clinicians monitoring and diagnosing HIV-DR at the earliest will be instrumental in preventing of resistance.
References:
UNAIDS Fact Sheet (2016).
Annual Report 2015-16 NACO
http://www.naco.gov.in/upload/2016%20Data/Annual%20Report/Annual%20Report%202015-16_NACO.pdf(accessed on 17.11.2016 )
Clavel, François, and Allan J. Hance. “HIV drug resistance.” New England Journal of Medicine 350.10 (2004): 1023-1035.
Balakrishnan, Pachamuthu, et al. “HIV-1 drug resistance among drug-naïve and HAART treated patients in India: Current status.” Regional Health Forum. Vol. 15. No. 1. 2011.
Naik, Shweta, and B. R. Das. “New WHO Guidelines: Implications on Therapeutics and Monitoring of HIV Infections.” HIV: Current Research 2016 (2016).
Authors
Dr. Shweta Naik (MD, Microbiology) Research Scientist, SRL, R&D SRL Ltd, Mumbai Reference LabDr. B. R Das, PhD Advisor and Mentor, Research & Development, Centre of Excellence in Molecular Pathology and Clinical Research Services SRL Limite