Understanding Lupus: For Beginners
WHAT IS LUPUS?
Lupus or systemic lupus erythrematosus (SLE) is an inflammatory connective tissue disease affecting multipe organs of the body. SLE is a type of autoimmune disease characterised by widespread activation of the immune system, with Tcell-Bcell interaction, auto-antibody generation, immune complex formation and deposition and deposition.
WHAT CAUSES LUPUS?
Research is still going on studying the causation for lupus. While no definite single cause has been found, various hypothesis do exist. Studies have shown female hormones, genetic susceptibility, smoking, mutations in DNAse1 enzyme and many more factors to be associated with lupus.
HOW TO DIAGNOSE LUPUS?
Wait! Don’t jump your answer to blood tests! Lupus is a great masquerader. It can evade detection- not only from the general public but also from many busy clinicians- unless it flares to a life threatening form. Just remember the basic principle: it can affect all organ systems of the body.
So, if you find a female patient of reproductive age with complains affecting more than one organ system, thi nk of lupus as a differential. The symptoms may range from:
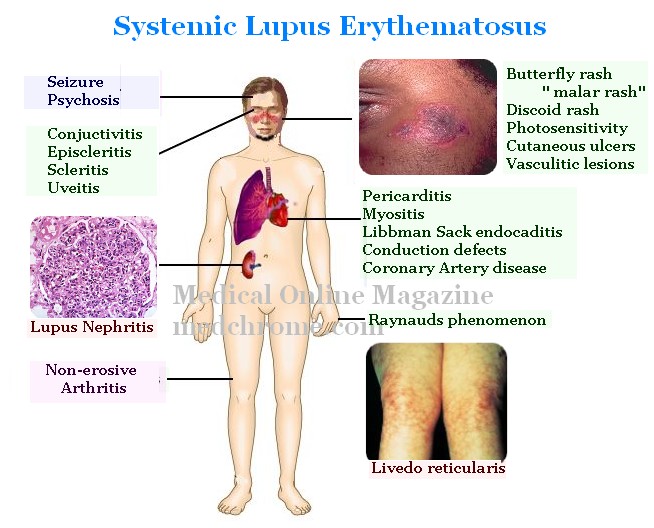
Fever (usually low grade), fatigue, excessive hair loss

Skin rashes: -Seen in 70%. Classical butteryfly rash (35%), discoid rash, cutaneous ulcers and vasculitic lesions. Skin problems are more when exposed to sun (photosensitivity)

Joint pains:- Seen in 90%. It can present in any pattern but the most common pattern is that of rheumatoid arthritis adding to the confusion. Joint involvement in lupus is without erosions on xray and the deformities, if present, are correctable (Jaccoud’s arthritis). And yes, the pains are inflammatory type (morning stiffness, swelling, redness, improvement with activity)
Respiratory symptoms: – dry cough and insidious onset gradually progressive dyspnea indicative of associated ILD or pleural effusion
-chest pain: pleurisy
-hemoptysis: alveolitis, diffuse alveolar hemorrhage, associated thrombocytopenia
– pulmonary infections: usually a complication of treatment but is most common pulmonary pathology in lupus-not to be forgotten!
Cardiovascular: all layers and structures you know in the heart can be affected:
pericarditis: chest pain, dyspnea
-myocarditis: palpitations, dyspnea, dizziness due to low blood pressure
-endocarditis: libbmann sacks endocarditis
-coronary artery disease: MI and angina are more frequent in patients with all connective tissue diseases including lupus.
-conduction system: heart blocks (especi ally congenital heart block in neonatal lupus!)
Renal: The most popular, though not the most common, organ involved in lupus. Affects 50% during the first year of diagnosis. Lupus affects kidneys in various severities. Exact confirmation andclassification of severity needs kidney biopsy. Patients may have features of renal failure including decreasing urine volume, dark coloured urine, edema etc. However, it is important to identify patients with early renal involvement of better outcomes. And most of those with early renal disease are asymptomatic from renal point of view.
CNS: Again, in CNS, lupus can have myriad of presentations! Seizures and psychosis are the most common ones. However, patient may present with parasthesia, weakness, hemiparesis, transverse myelitis, mononeuritis multiplex etc..
Hematological: Patients usually have cytopenias and are usually detected on routine investigation. However, they may present with excessive bleeding (thrombocytopenia), recurrent infections and fever (leukopenia) or fatigue, palpitations, exercise intolerance (anemia)
Eyes: conjuctivitis, episcleritis, scleritis, uveitis and even CRAO and CRVO related to anti-phospholipid syndrome- bascially a history of painful red eye!
The clinical features have always been confusing! And it would seem anything can be lupus! It’s the constellation of the symptoms rather than a single symptom, that guides us to the diagnosis. To make it much simple and pragmatic, the symptoms can be divided into ‘life threatening’ and ‘non-life threatening’ lupus.
Life threatening lupus:
1) CNS lupus
2) Lupus nephritis Class III and IV
3) Diffuse alveolitis or Diffuse alveolar hemorrage
4) Severe cytopenias
5) Mesentric ischemiaNon-life threatening lupus:
1) Musculoskeletal
2) Mild cytopenias
3) Cutaneous
The diagnostic workup and treatment should be fast and aggressive in cases of life-threatening lupus. However, in non-life threatening ones, a routine outpatient based treatment might suffice.
We will come in another session on approach to treatment of each of the categories of lupus patients.
Thank you.

Article By-
Dr Binit Vaidya,
MBBS, MD( AIIMS), FACR


2 Comments
It is very informative article. Thank you Doctor.
It was a nice clear publication on SLE.
I’m waiting for the treatment part as well.
Can I get the updates if I subscribe ?
Comments are closed.