Vitamin A : Sources, Metabolism and Deficiency
“A Severe Drought in Kenya wiped out a family’s yam crop, their primary staple food. Within several months, a 3 yr Old child in the family began to complain of being unable to see very well specially at dusk and night. Also, the child’s eyes were red due to constant rubbing because of dryness.”- Kaplan Biochemistry Lectures
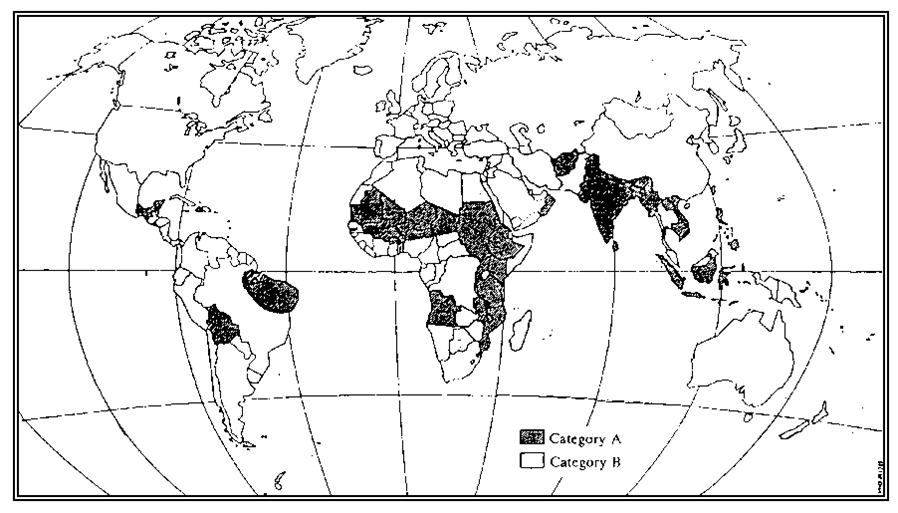
Magnitude of Problem-
Clinical and subclinical VAD are problems in at least 75 countries.
Clinical VAD occurs mainly in countries in Southeast Asia and sub-Saharan Africa. Severe VAD – refugee settlements and in displaced populations
Improving the vitamin A status of children with deficiencies (aged 6-59 mo) can reduce measles and diarrhea mortality rates by 50% and 33%, respectively, and can decrease risk rates from all causes of mortality by 23%.

Developing countries –
Estimated 250 million children are at risk for vitamin deficiency syndromes.
Up to 10 million malnourished children, develop xerophthalmia and have an increased risk of complications and death from measles.
Each year, 250,000-500,000 vitamin A-deficient children become blind every year, half of them dying within 12 months of losing their sight.
WHO Fact sheet
Dietary Source
Animal foods-
- Liver, Eggs, Butter, Cheese
- Whole milk, Fish and Meat.
- Fish Liver Oil – richest source.
Plant Foods- Provitamins
- Green leafy vegetable- spinach and amaranth
- Green and yellow fruits and vegetables- Papaya, mango,pumpkin and roots like carrots
Fortified foods-
▫Vanaspati, Margarine, Milk
1 Retinol Equivalent = 1 μg Retinol = 6 μg beta-carotene = 12 μg of other carotene
1 IU= 0.3 μg of Retinol.
Metabolism
Absorption ,Bioavailability and Transport
70-90% percent of vitamin A from the diet is absorbed in
the intestine.
Retinol-binding protein (RBP) is the specific carrier used
to transport all-trans retinol in the plasma.
The all-trans isoform accounts for more than 90% of all
plasma vitamin A .
Retinol + RBP= holo-RBP.
Holo-RBP + Transthyretin (TTR- prealbumin)- not filtered
by the glomerulus, but instead freely circulates
throughout the plasma
Storage
50 to 85% of the total body retinol are stored in the liver in hepatic stellate (star-shaped) cells along with droplets of lipid.
Over 90% – stored in the form of retinyl esters + FAOnce hepatic stellate cells are saturated with all the retinol -hypervitaminosis can result.
beta-carotene, can be stored in adipose cells of fat depots throughout the body .
Excretion –
Via- kidneys mainly via renal catabolism and glomerular filtration .
Renal disease
elevated serum levels of RBP and retinol
must be more aware of vitamin A toxicity.
Roles of Vitamin A-
- Vitamin A is essential to vision -production of retinal pigments for vision in dim light
- Role in gene expression and transcription, that regulates cell growth and differentiation.( Acts like Steroid Hormone)
- Retinoic acid is especially important in heart, eye, lung and ear development .
- The development of gap junctions between cells is also affected by retinoic acid. Regulation- Leucopynes
- Key role in glycoprotein synthesis ( Retinyl Phosphate) ,mucopolysaccharides and Transferrin
- Reproductive processes (spermatogenesis) &, bone development, along with maintenance, and immune system function are dependent upon different isoforms of vitamin A.
- Integrity of glandular & epithelial tissue which line Intestinal, respiratory & urinary tract, skin & eyes. testicular & vaginal epithelium.
- 8. Vitamin A also has antioxidant properties. ↓ incidence of lung, breast, oral, esophageal, & bladder cancers.

The RDAs of vitamin A for various age groups are as follows:
Infants aged 1 year or younger – 375 mcg
Children aged 1-3 years – 400 mcg
Children aged 4-6 years – 500 mcg
Children aged 7-10 years – 700 mcg
All males older than 10 years – 1000 mcg
All females older than 10 years – 800 mcg
Risk Factors for Vitamin A deficiency-
Intake Diarrhea, worms (ascaris) & other intestinal disorders impair vit A absorption
Measles, respiratory tract infection & other febrile illness ↑metabolic demands.
Protein Energy Malnutrition (PEM), Zinc & Iron deficiency impairs utilization & transport of Vit A.
toddlers and preschool children living below the poverty line.
Subclinical forms of VAD
Without any symptoms
Higher risk of developing respiratory and diarrheal infections
The growth rate is decreased, and bone development is slowed.
The patient may also report increased fatigue, as a manifestation of VAD anemia.
Occular Sign: WHO classification of Xeropthalmia
Primary signs:
X1A Conjunctival xerosis
X1B Bitot,s spots
X2 Corneal xerosis
X3A Corneal ulceration (1/3rd)
Secondary Signs:
XN Night blindness
XF Fundal changes
XS Corneal scarring

Extra-ocular manifestations:
Phrynoderma: scaly & toad like skin- Follicular hyperkeratosis
Renal & vesical calculi.
Atrophy of germinal epithelium interfere reproductive functions
Dry skin, Dry hair, Pruritus, Broken fingernails
Excessive deposition of periosteal bone secondary to reduced osteoclastic activity
Anemia
Keratinization of mucous membrane
Impairment of the humoral and cell-mediated immune system.
PREVENTION-
- Improvement of diet :
- adequate & regular intake of foods rich in vitamin A and Food Fortification.
- ↓contributory factors eg. PEM, diarrhea, respiratory infection & measles.
- Regular Vit A supplementation: Vit A can be stored in body for 6-9 months administer a single massive dose of 2 lakh IU vit A orally every 6 months to (preschool children/ 1-5 yrs) ½ the dose to (6 months to 1 yr) of age.
- In measles, severe PEM 2 doses oral for 2 consecutive days. Persistent diarrhea or prolonged febrile condition: one dose in each episode (least 1 month interval)
- During pregnancy (not >300 mug retinol/day): ↓ maternal morbidity & ↓ perinatal mortality.
- High dose at Post partum period: ↓ mortality in 1st 4 months of life.
- Consumption of Vitamin A rich food
- Kitchen garden: to grow vit A rich foods.
3 doses at 0, 1 & 30 days
50,000 for < 6 months, 1 lac 6-12 months & 2 lac unit in children >1 yr
Same dose repeat next day & repeat at 4 wks
Local t/t of eye:
- Antibiotic drops/ ointment X 3 day,
- atropine drops X 1 day,
- padding for corneal ulcer.
Vitamin A toxicity
Continous Intake of 15 X RDA
Acute/ pseudotumor cerebri (Intra Cranial Pressure ↑ICP):
headache, vomiting, dizziness, ↑ant. fontanel, papilledema.
Chronic intoxication causes:
nausea, vomiting, anorexia & sleep disorders
skin desquamation → Dermatitis
Enlargement of Liver and Spleen, hypolastic anemia
benign intracranial hypertension
Bone pain, Diarrhea
Teratogenic to fetus:
craniofacial malformation in fetus of mothers on oral retinoid for acne.
Investigations for VAD-
- A serum retinol study- costly but direct measure using high-performance liquid chromatography. < 0.7 mg/L in children-fluorometry, spectrophotometry
- A serum RBP study -easier to perform ,less expensive , RBP is a protein and can be detected by an immunologic assay.
- A zinc level is useful because zinc deficiency interferes with RBP production.
- An iron panel is useful because iron deficiency can affect the metabolism of vitamin A.
- Albumin levels are indirect measures of vitamin A levels.
- An electrolyte evaluation and liver function studies should be performed to evaluate for nutritional status.
- Imaging Studies -In children, radiographic films of the long bones may be useful when an evaluation is being made for bone growth and for excessive deposition of periosteal bone.
Procedures
Dark-adaptation threshold should be tested.
Recommendations-
- The American Academy of Pediatrics has recommended vitamin A supplementation for infants aged 6-24 months who are hospitalized with measles and for all hospitalized children older than 6 months.
- The WHO – UNICEF joint statements recommends -vitamin A be administered to all children, especially those younger than 2 years, who are diagnosed with measles.
- A Cochrane Database of Systematic Reviews article concluded that daily treatment with 200,000 IU of vitamin A for at least 2 days reduces mortality rates in Measles children less than 2 yrs.
- A more recent Cochrane Database of Systematic Reviews article, including 43 randomized trials representing 215,633 children, provides strong support for the importance of vitamin A supplementation in preventing childhood mortality.
- A single dose of vitamin A improves haemoglobin concentration, retinol status and phagocytic function of neutrophils in preschool children.
- A substantial reduction (40 percent) in pregnancy- related mortality was observed among the women who received vitamin A or beta-carotene supplements on a weekly basis before, during, and after pregnancy (West et al, 1999)
Vitamin A and its derivatives being used in
- Acne
- Psoriasis
- Treatment of Corneal Ulcer
- Role of Vitamin A as anti-oxidant is being studied.
- Studies going on to see if Vitamin A is solution to cancer- specially Breast, lung and Prostate Cancers.