Vitamin D deficiency: Clinical Significance and Diagnosis
Vitamin D: A Brief Glimpse of the Basics
Vitamin D refers to a fat soluble substance which enhances the intestinal absorption of calcium, iron, magnesium, phosphate and zinc. The biologically important compounds in this group are vitamin D3 (also known as cholecalciferol) and vitamin D2 (ergocalciferol). Cholecalciferol and ergocalciferol can be ingested from the diet and through Vitamin D supplementation. Very few foods contain vitamin D, the dermal synthesis of vitamin D from cholesterol is dependent on sun exposure (specifically UVB radiation). Hence, it is often referred to as the “sunshine vitamin”.
The Multi faceted systemic role played by vitamin D
The essential function performed by vitamin D in maintaining adequate and optimum bone health has been extensively researched and well proven. The link between low vitamin D levels and bone disorders like osteomalacia, rickets and osteoporosis; is well established. However, the medical fraternity is now discussing with renewed interest; the fact that vitamin D also plays a pivotal role in several non-skeletal functions such as maintenance of cardiovascular health, endocrine regulation, neoplastic diseases and cellular growth.
Substantial clinical evidence has established a strong link between vitamin D deficiency and many chronic diseases including hypertension, cancer, diabetes, and cardiovascular disease. Clinical studies have also reported cross-sectional associations between lower vitamin D levels and plasma renin activity, blood pressure, coronary artery calcification, and prevalent cardiovascular disease.
Vitamin D concentrations of >75 nmol/L (30 ng/mL) regulate optimum cell growth and prevent cells from becoming autonomous and developing into unregulated cancer. Vitamin D deficiency has thus been related to breast, prostate, and colon cancer. The elucidation of this multi faceted role played by vitamin D, in health and in disease, has attached unprecedented value to the laboratory testing of vitamin D levels for the diagnosis and therapeutic monitoring of vitamin D deficiency.
Vitamin D deficiency: Global and Indian Statistics
The Global Picture
As per data published by BMJ in early 2015, Vitamin D deficiency is the most common nutritional deficiency worldwide in both children and adults. In the US and Europe, >40% of the adult population >50 years of age is vitamin D-deficient. Levels of serum 25-hydroxyvitamin D consistent with vitamin D deficiency have been reported in 48% of pre-teen white girls, 52% of adolescent Hispanic and black American boys and girls, and 32% of healthy young adults. In Tibet and Mongolia, vitamin D deficiency leading to clinical rickets is described in 60% of infants. In the Middle East, a high prevalence of rickets and osteomalacia has been described in women and their infants.
The Indian Scenario
A leading national daily reported the findings of an epidemiological study which stated that nearly 80% of Indians suffer from vitamin D deficiency. Indian clinical studies which measured serum 25(OH) D, using sensitive and specific assays in apparently healthy subjects have confirmed hypovitaminosis in up to 90 per cent of study subjects. Contrary to the popular western belief that the incidence of vitamin D deficiency is low in India, several Indian studies have confirmed widespread vitamin D deficiency in Asian Indians of all age groups including; toddlers, school children, pregnant women, neonates and adult males and females residing in rural or urban areas. It’s indeed an irony that in a country like ours, with abundant sunshine, a large chunk of the common masses shows deficiency of the ‘sunshine’ vitamin!!!
The probable causes of vitamin D deficiency in a “sunshine” country like India
Limited sun exposure due to cultural and lifestyle practices, dark skin color, very hot climate in several parts of the country, prolonged breast feeding without vitamin D supplementation, limited outdoor activities, obesity, lack of vitamin D fortification of food, poor socieconomic conditions, poor diet, certain hormonal disorders, the use of certain medications, malabsorption syndromes, inadequate calcium intake, lactose intolerance and certain genetic disorders; comprise some of the commonly known and reported reasons for vitamin D deficiency.
SRL in-house pan-India data on vitamin D tests performed during 2012—14
During the period 2012—14, across India, SRL labs performed a total of 316025 Vitamin D tests. Of these, below normal levels of vitamin D were detected in a whopping 86.20% samples (n=272444).
Pan India analysis of SRL test result data for the period 2012-14, demonstrated that out of 183419 samples tested for females; a total of 76.24% samples from females (n= 139838) had deficient vitamin D levels. SRL labs also performed Vitamin D testing for a total of 132606 males across India, during 2012—14. Of these, 80.63% (n=106920) samples showed vitamin D levels below normal. The results have been illustrated below.
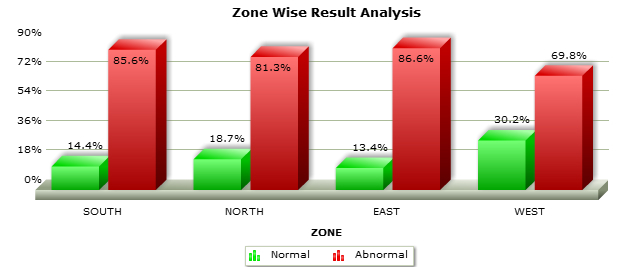
Zonal Analysis of Male and Female tests for Vitamin D
Women
Men
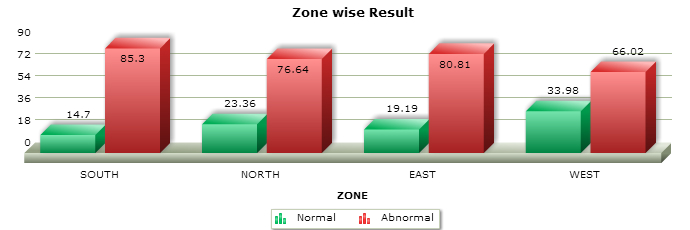
As per this data, the proportion of below normal vitamin D test results for each geographic zone in the country has also been depicted in the images below, for male and female categories. A zonal analysis of the samples tested for vitamin D has been presented below. In both the gender categories, the southern and eastern zones of the country showed the highest number of vitamin D deficient samples.
Age wise break up of Vitamin D deficient samples
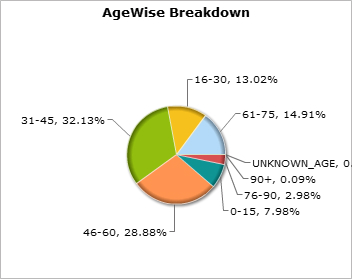
Women
Men
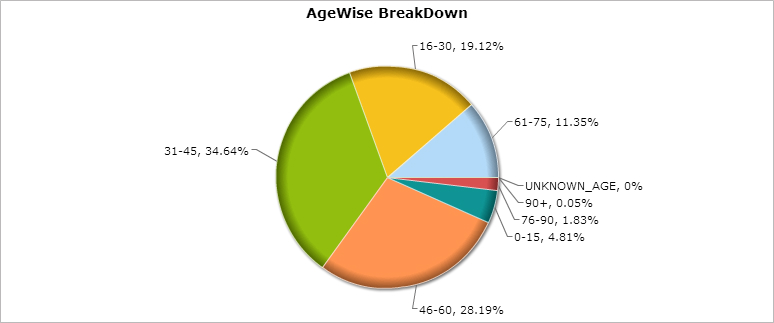
Samples from males showing a deficient vitamin D status were predominantly in the age groups of 31—45 years (32.13%) and 46—60 years (28.88%). A similar pattern was seen in samples tested for females; with maximum percentage of deficient samples being reported in the age groups of 31—45 years (34.64%) and 46—60 years (28.19%).
Vitamin D with a special focus on Osteoporosis
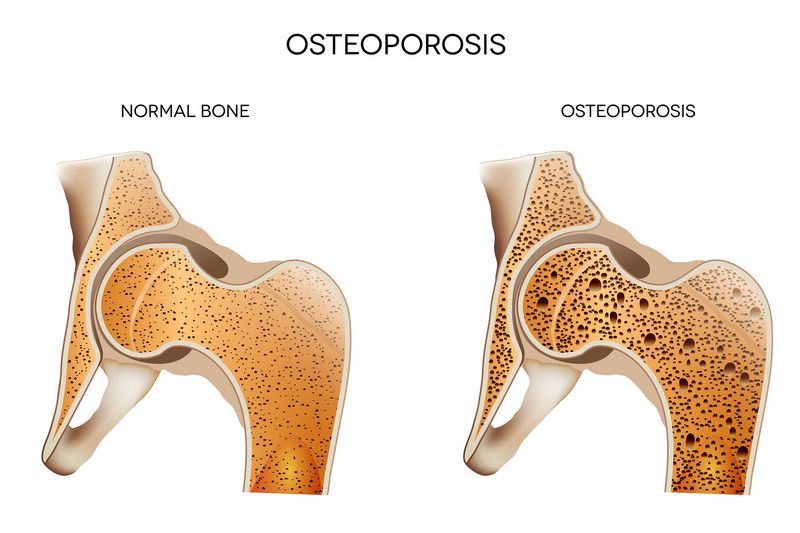
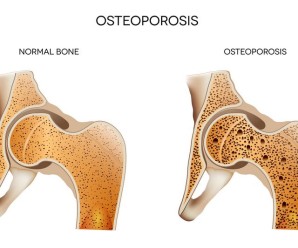
Osteoporosis typically refers to a condition wherein bones develop porosities, become brittle, weak and fragile; and are highly susceptible to fracture. Osteoporosis can be caused by a plethora of causes, beyond the scope of discussion here. However, one of he commonly noted contributing factors towards this disease is a low vitamin D level. In the absence of adequate vitamin D, calcium absorption from the gut and its deposition into the bones is hampered. As a result, it contributes to the reduced bone density and increased porosities noted in osteoporosis.
Key data highlights put forth by the International Osteoporosis Foundation (IOF) are an implied indicator of low vitamin D levels and low bone density more rampant among women all over the world as compared to men. Osteoporosis is estimated to affect 200 million women worldwide – approximately one-tenth of women aged 60, one-fifth of women aged 70, two-fifths of women aged 80 and two-thirds of women aged 90. Worldwide, 1 in 3 women over age 50 will experience osteoporotic fractures, as will 1 in 5 men aged over 50. 80%, 75%, 70% and 58% of forearm, humerus, hip and spine fractures, respectively, occur in women. Overall, 61% of osteoporotic fractures occur in women, with a female-to-male ratio of 1.6. By 2050, the worldwide incidence of hip fracture in men is projected to increase by 310% and 240% in women. Although low BMD confers increased risk for fracture, most fractures occur in postmenopausal women with moderate risk.
An IOF survey, conducted in 11 countries, showed denial of personal risk by postmenopausal women, lack of dialogue about osteoporosis with their doctor, and restricted access to diagnosis and treatment before the first fracture result in under diagnosis and under treatment of the disease.
In conjunction with clinical features and radiological examinations, Vitamin D testing is a frequently performed and crucial part of the biochemical work up of osteoporosis and other bone and joint related disorders.
Authors: