Diagnosis of Extrapulmonary Tuberculosis: Need of the hour
Editor
March 23, 2016
7 min read
1904 Views
The burden of tuberculosis (TB) in India is the largest in the world with around 23% of the global 9.6 million affected people in 2014.While pulmonary tuberculosis (PTB) is the most common presentation, extrapulmonary tuberculosis (EPTB) accounts for a significant proportion of tuberculosis cases worldwide. In India, 10-15% of cases in immunocompetent individuals are EPTB, but this number could go up to 50 % in HIV infected persons.
Clinical manifestations of EPTB are varied as any organ system may be involved though the most common presentations seen include TB lymphadenitis, pleural effusion, abdominal TB, bone and joint TB,miliary TB, meningeal TB and genitourinary TB. Depending on the organ affected, the patient will have symptoms ranging from minor swelling of lymph nodes to breathlessness in pleural effusion and may even present with convulsions, headache, fever, neck stiffness and mental confusion in cases of neurological TB. Constitutional symptoms in patients with EPTB include fever, anorexia, weight loss,malaise and fatigue. In India patients with EPTB, may present with pyrexia of unknown origin (PUO) as the only diagnostic clue in them, especially when the disease is located at an obscure site. Though EPTB is less infective as compared to PTB, EPTB has more severe consequences as serious sequelae can cause significant morbidity and even mortality. Recent reports have highlighted the fact that drug resistance(DR) has been noted in a significant number of EPTB cases which may impact the efficacy of standard treatment regimes. Accurate and rapid laboratory tests have gained importance as EPTB remains a challenge that can perplex even the most experienced clinicians to diagnose on clinical grounds alone.
Laboratory diagnosis of EPTB:
The diagnostic algorithm for EPTB includes microscopy, culture, nucleic amplification platforms and immunology based tests. Definitive diagnosis of TB depends on the culture of Mycobacterium tuberculosis (MTB) from the specimen obtained from the patient.
Sample collection for EPTB is often difficult as clinical samples have to be obtained from relatively inaccessible sites requiring invasive procedures for the best results. Deep seated sites of involvement in bone or intestine may require biopsies under guidance of ultrasound, computed tomography (CT), or endoscopic ultrasound whereas in superficial TB lymphadenitis, fine needle aspiration biopsy of affected lymph nodes may suffice. Pleural effusion requires tapping for collection of pleural fluid. Tuberculosis meningitis is diagnosed by examination of cerebrospinal fluid obtained by lumbar puncture.
These critical samples however are most often paucibacillary and yield of MTB is generally low from tissue and fluid specimens. Multiple samples may assist in enhancing diagnostic performance especially in patients with urinary tract TB and cerebrospinal fluid (CSF), but it is not feasible to repeat invasive procedures for obtaining specimens.Tissue biopsy is a better sample than fluid aspiration,yielding positive culture results more often.
Microscopy:
The simplest and the most inexpensive test for diagnosing TB is by microscopy.
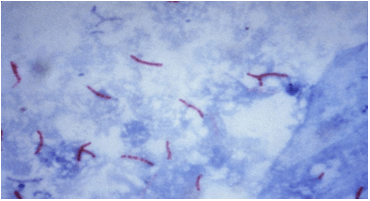
Ziehl-Neelsen staining, though can be performed at the primary care level, is relatively insensitive due to the paucibacillary nature of EPTB and cannot rule out the disease. Fluorochrome-based staining is 10% more sensitive but requires considerable expense and technical expertise. Recently, use of Light emitted diode (LED)microscopy has shown greater diagnostic accuracy over conventional methods.
Histopathology examination of tissue biopsy showing presence of granulomas, caseation, and demonstration of acid fast bacilli have been commonly used to define a positive test. However, nontuberculous mycobacteria (NTM) disease, fungal infections, brucellosis, or syphilis also cause granulomas. In addition, loss of host immune function can result in histopathologic findings demonstrating greater suppurative response and less well-formed granulomas, so cautious interpretation is required in both positive as well as negative findings.
Microscopy cannot distinguish MTB from NTM, nor viable from non-viable organisms, or drug-susceptible from drug-resistant strains which is a major drawback in the current scenario of DR strains.
Culture and drug sensitivity:
The gold standard for TB diagnosis remains a positive culture report which indicates an active infection. Culture is more sensitive than microscopy and allows differentiation of M. tuberculosis from NTM. Liquid culture increases the case yield by 10% over solid media, and automated systems can generate reports in days rather than weeks, overcoming the drawbacks of solid culture. Culture remains the only technology that can detect resistance to all major TB drugs and provides a definitive diagnosis of drug-resistant TB. Culture is much more complex, expensive and mandates appropriate biosafety measures compared to microscopy and is difficult to implement at primary care level.
Molecular tests :
Nucleic acid amplification tests (NAATs) overcome the shortcomings of culture and enable rapid diagnosis, which is of tremendous value in life threatening diseases such as TB meningitis. Enhanced sensitivity by NAAT detects infections missed by microscopy in paucibacillary samples of EPTB. Genexpert:Xpert MTB/RIF assay, a novel, automated, cartridge-based NAAT, introduced for detecting MTB complex and rifampin (RIF) resistance has now been recommended by World Health Organization over conventional tests for diagnosis of TB in lymph nodes and other tissues, and as the preferred initial test for diagnosis of TB meningitis. Sensitivity of Xpert MTB/RIF in testing body fluids, however, is very low. Due to the high specificity but low sensitivity, a positive NAAT result can be considered a presumptive case, whereas a negative NAAT cannot be relied upon to exclude the diagnosis in body fluids.The major drawback of NAAT is that it is unable to differentiate between viable and nonviable MTB.
DNA sequencing can be used for evaluating suspected drug-resistant MTB isolates with discordant results for phenotypic susceptibility and rapid molecular testing.
Newer tests in the pipeline include TB-LAMP is a new manual TB detection method based on the novel loop-mediated isothermal amplification (LAMP) platform could be implemented in place of microscopy to improve the accuracy of TB detection at microscopy centres. Recent papers have noted that line probe assay (LPA) technology may prove to be of utility in EPTB samples, but it has not been validated for the same. LPA can be used to diagnose drug resistance if MTB has already been isolated from EPTB samples which allows rapid testing of second line drugs.
Supplementary tests :
Adenosine deaminase (ADA) is widely used as a biomarker in body fluids for the diagnosis of EPTB. Activity of ADA increases in TB patients because of the stimulation of T-cell lymphocytes by mycobacterial antigens. It has been proposed to be a useful surrogate marker for TB in body fluids,such as pleural, pericardial, and peritoneal fluid, although possible false-negative and false-positive results should be considered.
Immunological tests like Tuberculin skin test (TST) and IFN-γ releasing assay (IGRA) may be supportive for diagnosing EPTB, but have limited diagnostic value. Interpretation of TST reactivity can be complicated by cross-reactivity with previous Bacille Calmette–Guerin vaccination or latent TB infection. Factors such as HIV infection, poor nutritional status, recent viral or bacterial infections, or vaccination with live virus can reduce response to the TST. Similarly use of IGRAs for active TB will result in unacceptably high rates of false positive results because IGRAs cannot separate latent TB infection from active TB disease, and a large proportion of the Indian population is latently infected.
Antibody detection-based serological tests are banned by the Government of India since 2011 as they have variable sensitivity and specificity .
The Diagnosis of EPTB: In a nutshell
To summarize, NAATs have considerable advantages over conventional tests offering speed of diagnosis and detection of drug-resistant TB. However, culture remains the most sensitive technique for EPTB samples and for detection of DR-TB.The diagnostic accuracy could increase further when the results of the biopsy histology and NAATs are combined with those of culture.
In conclusion, EPTB can affect any part of the body, with misleading symptoms mimicking other pathologies. This leads to diagnostic delays or even missed diagnoses. Given the challenges obtaining an adequate sample for culture in EPTB, there is a need to raise clinical awareness around the challenges posed by EPTB and the advances in laboratory medicine for diagnosing EPTB.
Dr. Shweta Naik (MD, Microbiology) Research Scientist, SRL, R&D SRL Ltd, Mumbai Reference LabDr. B. R Das President-Research & Innovation, Mentor-Molecular Pathology and Clinical Research Services SRL R&D, Mumbai
Medchrome – Online MedicalMagazine has been publishing academic medical and health related articles since 2009. Medchrome Networks include Medchrome Videos, Medchrome Answers and has collaboration with Epomedicine – Mnemonics, Simplified Concepts and Thoughts.
DISCLAIMER: The Articles and information on Medchrome are NOT intended as a Medical advice. Any information, protocols, illustrations and products contained in this website is for INFORMATION and EDUCATION PURPOSE only. Please consult a healthcare profession for any medical advice.